

![]()
![]()
Food Safety Focus (2nd Issue, September 2006) – Food Safety Platform
Hazard and Risk in Food Safety (Part II)
Reported by Dr. Anna TANG, Research Officer,
Risk Assessment Section, Centre for Food Safety
Introduction
As mentioned in Part I, hazards and risks are part of everyday life. For food, we are constantly exposed to various materials, natural or synthetic, that are potentially hazardous to us which may be present unintentionally due to contamination or added intentionally for reasons like improving texture and taste. With advances in modern technology, we are able to detect these materials at a lower and lower level. While achieving zero tolerance for all food hazards is not realistic, our exposure to these hazards will determine if our health is at risk.
The Effect of Dose
Too much of a good thing may be bad. A little of a bad thing may not be as bad as we may think. Dose, i.e. amount of substance we are exposed to and the duration of exposure determines whether something is a poison. Taking oxygen as an example, it is a good thing because we all need it for survival. However, oxygen concentration above 60 % may cause irritation to lungs and affect respiration. High oxygen concentration over a prolonged period can lead to oxygen poisoning, causing convulsions and unconsciousness. Similarly, vitamins, which are essential to our life, can be considered as poisons when they are taken in excess because harmful effects to our bodies may occur.
Safety Reference Values
In food safety control, safety reference values are established as guidelines for a safe level of intake. They represent the amounts of a substance that can be ingested by a person over a period of time without appreciable health risk. When considering acute or immediate effects, an "acute reference dose" is used as a reference for the safe ingestion of a substance over a short period of time (e.g. 1 day). When considering chronic or long term effects, values such as "acceptable daily intake" (ADI) for food additives and "tolerable daily/weekly/monthly intake" for food contaminants over a lifetime period are usually taken as reference. Since these chronic reference values are determined based on lifetime intake, an occasional exposure above these values would not cause harm to health provided that the level is not high enough to cause immediate effects and its intake is not over in the long term.
Safety reference values generally used are those established by the Joint FAO/WHO Expert Committee on Food Additives (JECFA) and the Joint FAO/WHO Meeting on Pesticide Residues (JMPR). These organizations establish safety reference values for food additives and contaminants following safety assessments that take into account results of animal studies and human data. An ample margin of safety is given to protect public health. Substances evaluated by the JECFA and the JMPR undergo a periodic review procedure to ensure that new scientific data are considered whenever available.
Mercury as an Example
Mercury is a heavy metal that may cause adverse health effects particularly to the nervous system of developing foetuses and children and the kidney. Dietary food items are the major source of mercury.
The risk associated with ingestion of mercury in food by Hong Kong secondary school students can be estimated by comparing the intake of mercury (i.e. the exposure) in this group of population with the appropriate safety reference value (in this case provisional tolerable weekly intake (PTWI) established by JECFA) (Figure 1). In general, the risk of an adverse health effect due to ingestion of a substance is considered as acceptable when the dietary intake is lower than the safety reference value.
Figure 1: Assessment on the Health Effects of Mercury in Food 
According to the food consumption pattern of Hong Kong secondary school students and the levels of mercury in food determined by laboratory analysis, the estimated dietary intakes of mercury for average consumers and high consumers among secondary school students were all below the PTWI (Figure 2). The risk of adverse health effects due to dietary intake of mercury is therefore low for this group within the population.
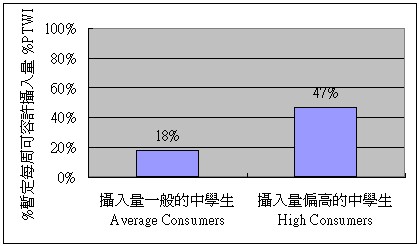 Figure 2: Dietary Exposure to Mercury among Secondary School Students Represented as a Percentage of PTWI Based on Results of Risk Assessment on "Dietary Exposure to Mercury in Secondary School Students" conducted by the Food and Environmental Hygiene Department
Figure 2: Dietary Exposure to Mercury among Secondary School Students Represented as a Percentage of PTWI Based on Results of Risk Assessment on "Dietary Exposure to Mercury in Secondary School Students" conducted by the Food and Environmental Hygiene Department